
Case Report | DOI: https://doi.org/10.31579/2690-1919/154
1 Department of Neurosurgery CHU Mustapha Bacha Algiers, Algeria.
*Corresponding Author: L. Atroune, Department of Neurosurgery CHU Mustapha Bacha Algiers, Algeria.
Citation: L. Atroune, Bouaita K., Midoune A., Benallag S., Habchi N., et.al (2021) Cutaneous Metastasis from Glioblastoma. J Clinical Research and Reports, 7(4); DOI:10.31579/2690-1919/154
Copyright: © 2021 L. Atroune, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 March 2021 | Accepted: 16 April 2021 | Published: 23 April 2021
Keywords: glioblastoma; cutaneous metastasis; scalp; anatomopathological examination; extracranial metastases; fronto-parietal; sarcomatous metaplasia; WHO
Extracranial metastases from glioblastoma multiforme (GBM) are rare, especially cutaneous metastasis. However, the metastatic mechanism of GBM remains unknown with no current consensus regarding the best therapeutic regimen.
We report the clinical, imaging and pathological features of a case of a 47 years old man with primary glioblastoma; who 12 months after receiving a macroscopically total resection and adjacent radiotherapy, developed scalp metastasis and subsequent multiple skin metastasis. We also discuss the details of this case in comparison with the previously reported cases in literature in terms of clinical presentation, lesions’ site, management and survival.
Extracranial metastases of glioblastoma are considered a rare entity with an incidence of 0.2 to 2% [1]. Given the aggressive clinical course of GBM, its low tendency to metastasize remains intriguing, The first case of extraneural spread of a malignant glial tumor was reported by Davis in 1928 [2], the first case of skin metastasis was reported in 1988 by shuangshoti [3]. The most common sites include the lung, liver, lymph nodes and long bones. However, around twenty cases of skin metastases from glioblastoma have been published until 2020. (table1) we can observe that skin and soft tissue metastases of GBM have occurred at the site of the craniotomy or the stereotaxic biopsy, and it appears that the presence of skin and soft tissue metastases is concomitant with intracranial recurrence; however it is not known whether the surgical technique plays a role in the dissemination or not.
We report the case of a 47-year-old man with a history of arterial hypertension under treatment, who presented with memory disorders associated to visual loss evolving since 02 months; A cerebral MRI showed an intra-axial left fronto-parietal lesion suggesting a glial tumor; A macroscopically total resection was performed; the anatomopathological examination revealed a grade VI glioblastoma according to WHO classification;
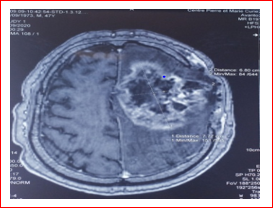
Afterwards the patient benefited from 30 sessions of radiotherapy (60gy), post-radiation MRI showed a recurrence of the fronto-parietal process of 68.8mm in diameter. (Figure 1)
One year after the first diagnosis of glioblastoma, the patient presented with erythematous pustulosis rash starting from the scalp near the surgical site, then generalizing to the whole body. (Figure 2)

With multiple homolateral cervical lymphadenopathy in the ultrasound (Figure 03) suggests a secondary origin, confirmed by echoguided puncture;

A biopsy of the scalp and the skin lesions was performed; the histological study with direct immunofluorescence and IHC profiling confirmed the skin location of glioblastoma.
The patient then received several sessions of chemotherapy such as temozolomide 400mg D1-D5 / 28 days and bevacizumab 10mg / kg.
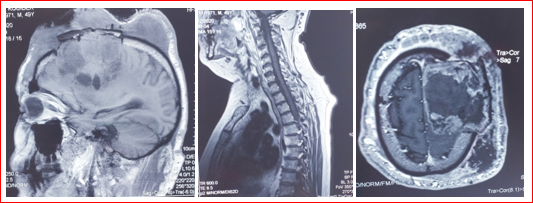
The cerebrospinal MRI revealed an advanced left frontal lobar glioblastoma, presenting a significant extension to the scalp; to the external auditory canal and the salivary glands through the craniotomy flap; with bilateral cervical lymph node invasion, left para-vertebral superficial muscle nodule secondary appearance; and osteolytic lesions of the vertebral body of T7 lateralized to the right and superomedial of the body of L2 (figure4);
Palliative treatment was therefore undertaken; however the patient succumbs to the endocranial and exocranial progression of the glioblastoma, 16 months after the first diagnosis of glioblastoma and 04 months after the appearance of extra cranial metastases.
Glioblastoma is a malignant astrocytic tumor that often affects men aged 45-55, with a survival rate of 10 months; Metastases of glioblastoma in the central nervous system (CNS) are frequent; on the other hand extra cranial metastases are very rare.
Given the aggressive clinical course of GBM, its low tendency to metastasize remains intriguing, some explain it by the short survival rate and the efficient immune response to malignant glial cells outside the CNS [4]; In their meta-analysis of 88 cases of metastatic GBM, Lun and al found a greater predisposition to extra-CNS metastases in young patients with an average age of 42 years [5], similar to the age of our patient;
Piccirilli and al report the most common sites of extra cranial metastases: lung and pleura 60%, lymph node 51%, bone 31%, while cutaneous are exceptional [6]; A meta-analysis of patients with extracranial metastases at any site found an average of 9 months between initial diagnosis and diagnosis of metastasis [7]. Our patient developed metastases approximately 12 months after the initial diagnosis;
In reported cases (Table 1), skin and soft tissue metastases of GBM have occurred at the site of the craniotomy [4] and that of the stereotaxic biopsy, However, it appears that the presence of skin and soft tissue metastases is concomitant with intracranial recurrence, the exact mechanism is unknown but it could result from the subcutaneous implantation of tumor cells during surgical excision by the dissemination of the cells along the pathway the procedure or by biopsy through the dura to the skin.
It is not known if the surgical technique plays a role; the GBM can be removed as a whole or by fragmentation, Intuitively, the second might be the most involved [8]; The majority of cases of extra cranial metastases of glioblastoma are postoperative following tumor resection or ventriclo-peritoneal bypass, but 10% of cases do not correlate with a neurosurgical intervention [9, 10].
The location along the operative site suggests that the metastasis mechanism is direct by seeding of the tumor, in particular when the metastasis appears on imaging just after surgery; other distant metastases can occur by different mechanisms of dissemination not yet understood but several hypotheses were put forward; the direct mechanism, vascular or lymphatic invasion, and the presence of molecular and genetic predisposing factors.
The direct mechanism represented by the locoregional dissemination by contiguity towards the scalp, would be the mechanism retained for our case.
The systemic dissemination is explained by two theories, first; lymphatic invasion even in the absence of any surgery; Louveau and al for the Kipnis laboratory [11] and Aspelund and al for the Alitalo laboratory [12] have demonstrated the existence of a lymphatic system in the meninges called the "Glymphatic system" along the superior longitudinal and transverse sinuses that drain to the deep cervical lymphatic system, which explains the frequency of cervical lymph node metastases [13], a secondary dissemination can be done via the systemic lymphatic vessels to give metastases at a distance including the skin as observed in our case for generalized skin lesions;
The second theory concerns the systemic dissemination by vascular invasion explained by the rupture of the blood brain barrier (BBB) possible even without surgery by epithelio-mesenchymal transformation [13]. In the normal case, glial cells cannot cross the blood brain barrier because of their molecular weight and cannot circulate in the blood because they are filtered by the immune system.
Liu and al. hypothesized that these cells suffer a process of epithelial-mesenchymal transformation (EMT), acquiring skills for migration, such as the production of metalloproteinases and proteases enzymes capable of degrading the basal capillary membrane, allowing the breaking of the BBB [14].
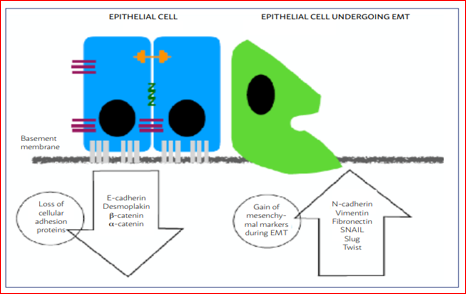
Some of the EMT markers are: loss of epithelial markers and acquisition of mesenchymal cells, rupture of the intercellular adhesion, change of the apicobasal polarity and remodeling of the cytoskeleton. These changes are associated with the increase of cell migration and resistance to anoikis (programmed cell death by detachment from the extracellular matrix) (Figure 5) [15].
This transformation can be an undesired consequence of the GBM treatment, particularly RT and chemotherapy with alkylating agents, due to its potential to induce mutations on glial cells [17]; but this transformation can be reversed at any time, stopping the migration process;
The passage of tumor cells known as circulating stem cells (SCSs) into the blood is carried out by the process of leukocyte extravasation (Figure 6) [18].
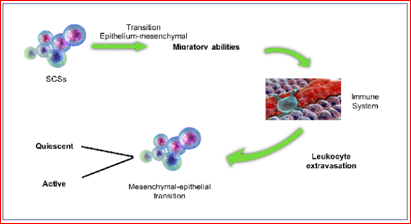
An example of the EMT/EMT process is the sarcomatous metaplasia. It is the acquisition of a sarcomatous phenotype by neoplastic glial cells, allowing the acquisition of extracellular matrix of proteins necessary for vascular invasion [17];
Once in the bloodstream, the SCSs incur a second filter: the immune system; As a result, in immunocompetent subjects, a large part of these cells ends up being detected and destroyed by the natural killer cells, while other subtypes escape the immune system by binding to blood components such as platelets to reach the connective tissue of the target organ where they may either stay quiescent until conditions become favorable for their activation, such as radiation-induced immune-suppression [19]; or active representing 5% of SCSs which have retained their renewal potential, which are very tolerant to hostile environments, host defenses and the suppression of growth factors
Quiescent cancer cells are usually resistant to chemotherapy [20]; and their evidence is confirmed by the work of Naumov and al, who have described that some cell lineages, including GBM, could not induce tumors in vivo for a long period [21]; The emergence of new technologies for detecting SCSs or even pieces of DNA from tumor cells in peripheral blood [22]; Müller and al published a study which demonstrated the presence of circulating cancer cells from GBM in the peripheral blood of patients. The cells were detected by an immunocytochemical method, by analysis of the glial fibrillar acid protein (GFAP), and its origin was confirmed by genomic tests (CGC and FISH); A total of 141 patients with GBM were tested, Thirteen tested positive before surgery; This shows that the GBM cell can spread regardless of surgery [23].
Almog and al. hypothesized that quiescent tumors suffer a stable genetic reprogramming when they pass to the rapid growth phenotype and they performed a wide transcriptional genomic analysis in search of the underlying molecular mechanism of these alternating states for various tumor histologies, including GBM; they found that the expression of ephrine tyrosine kinase receptor (EphA5), in particular, is significantly increased in quiescent GBM cells; this expression showed a correlation with the pathological degree, the lower their levels, the more advanced the tumor is[24]; Hence the interest of carrying out biomolecular and genetic studies to identify people at risk of developing metastases.
The management of metastatic glioblastoma is multidisciplinary including surgical excision first, followed by radiotherapy and chemotherapy as adjuvant treatment; as presented in the table 1, the majority of patients underwent surgery in combination with radiotherapy and/or chemotherapy [4]. Chemoradiation alone has also been used, but Senetta and associates found better local control with surgery plus radiotherapy compared with biopsy plus radiotherapy with adjuvant temozolomide [25]; Reviews of previous cases (Table 1) and Studies have shown that the average survival rate from the diagnosis of metastasis is 06 +/- 08 months, it can be prolonged by different aggressive treatments [7]; in our case the patient died 04 months after the diagnosis of metastases.

Due to the rarity of cases, there is no consensus on the treatment of metastatic GBM. The most frequently used drugs are temozolomide and nitrosoureas and Bevacizumab used as monotherapy or in combination [17].
Extracranial metastases from glioblastoma are rare and postoperative in the majority of cases. Nevertheless the pathogenesis of these metastases is not clear, several hypotheses have been put forward. Skin metastases are even more exceptional compared to other locations. Investigation and periodic monitoring are therefore required to detect and treat them early.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
